

Key highlights
Product specifications
| Compound Class | Selective Androgen Receptor Modulator (SARM) · Non-steroidal |
|---|---|
| Concentration | 25 mg/mL |
| Composition | USP-grade PEG-400 base, MK-2866 (≥98% purity) |
| CAS Number | 841205-47-8 |
| Chemical Formula | C19H14F3N3O3 |
| Molar Mass | 389.33 g/mol |
| Half-Life | ~24 hours |
| Synonyms | Ostarine, MK-2866, GTx-024, Enobosarm |
| Volume | 30 mL per bottle (750 mg total) |
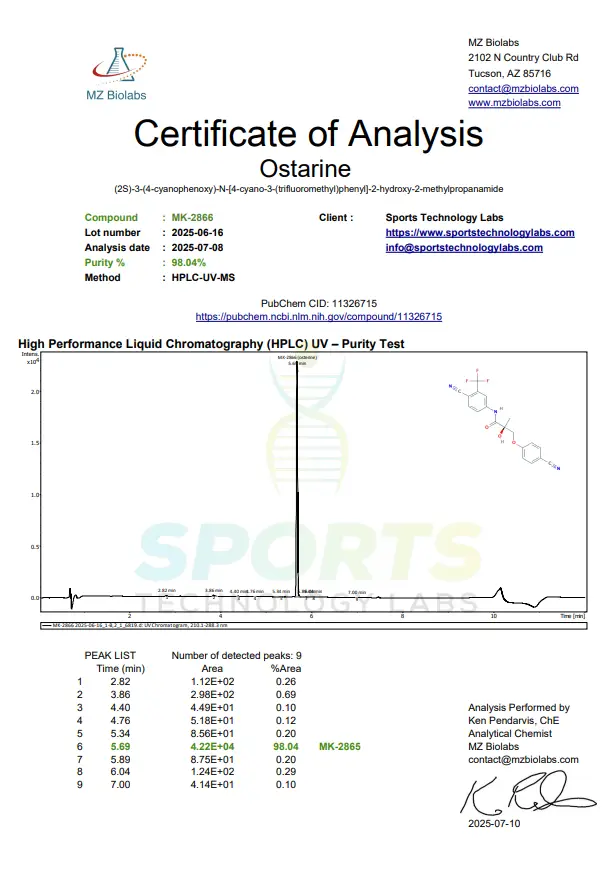
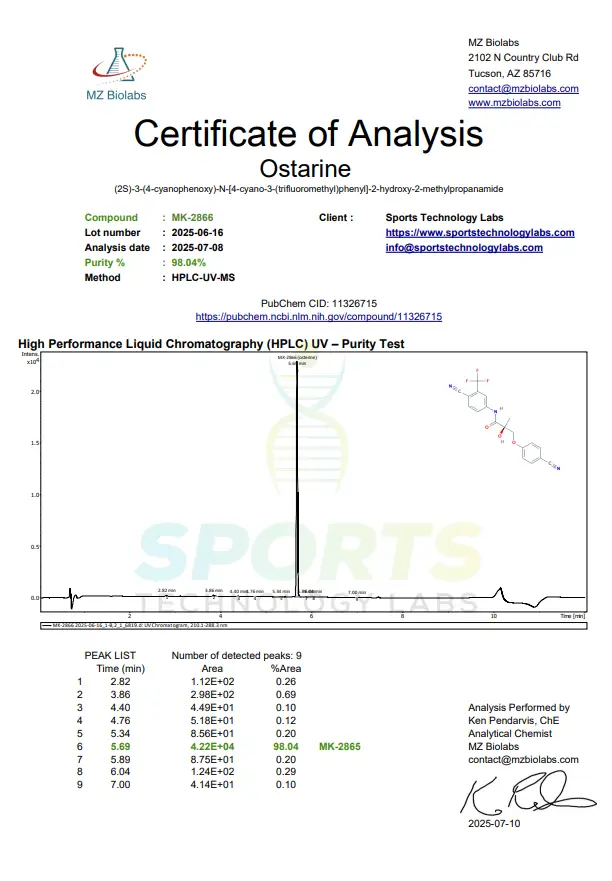
| Verified Purity | Batch-tested to 98.04% (HPLC) |
| Terms | For laboratory research use only. Not for human or animal consumption. |
Independently verified98.04% pure
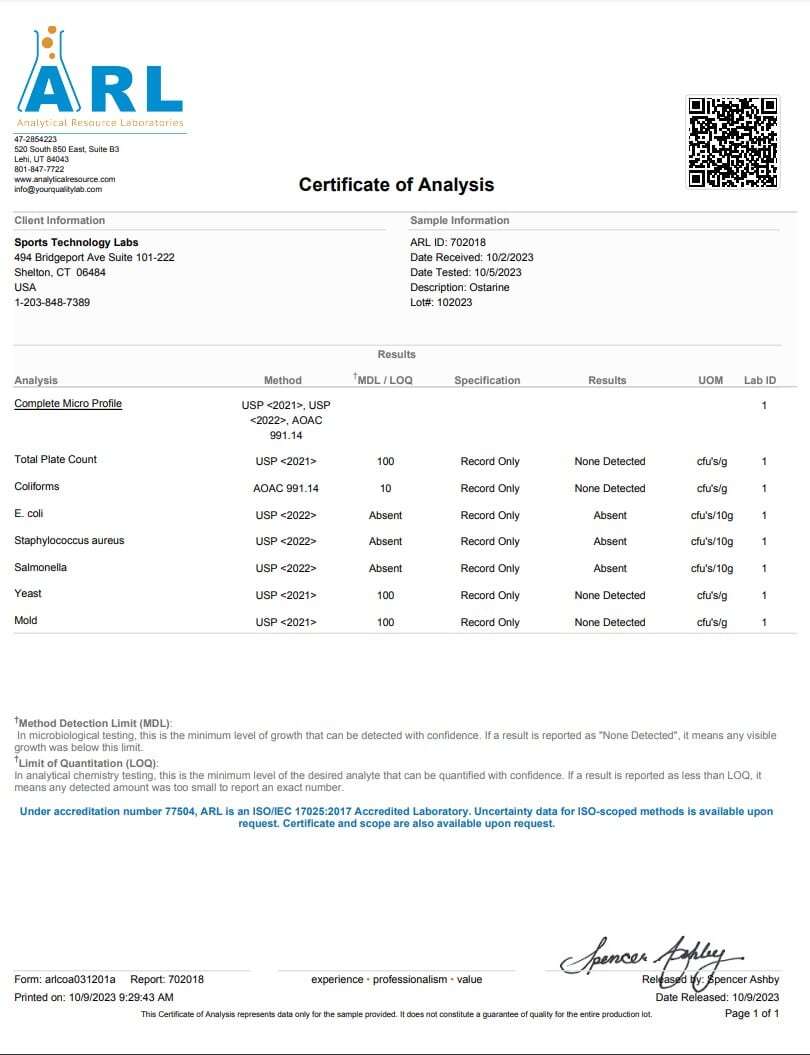
Every batch is analyzed by an accredited US third-party laboratory before it ships.
Purity and identity confirmed by MZ Biolabs (Tucson, AZ), a US DEA-licensed analytical facility, via HPLC purity analysis and mass-spectrometry identity confirmation under GLP standards.
Every COA is published openly, batch-dated, and matched to the product you receive — no login required.
Each bottle is formulated and verified for consistent label-to-bottle accuracy across studies.
Storage & handling
Built to preserve compound integrity throughout your research timeline.
- Storage: Keep in a cool, dry place away from direct sunlight to maximize shelf life.
- UV-resistant glass bottle with fixed glass dropper to minimize degradation and avoid plasticizer (BPA) leaching.
- Tamper-proof seal to ensure integrity in transit.
- Graduated 1 mL glass pipette included for precise measurement.
- Evaporation-resistant formulation and packaging for stable storage.
Why source Ostarine from Sports Technology Labs
Quality control across the research-compound industry is inconsistent, which makes third-party verification essential. A 2017 analysis published in JAMA examined 44 products marketed online as SARMs and reported wide gaps between labels and contents.
Source: Van Wagoner et al., JAMA, 2017 (ref. 2).
Verified by MZ Biolabs (Tucson, AZ), an accredited US laboratory, via HPLC and mass spectrometry.
Suspended in the highest grade carrier and bottled in America.
Prevents BPA leaching and avoids contamination from external tools.
Transparent business, standard payment methods, no misrepresentation.
What is Ostarine (MK-2866)?
Ostarine (MK-2866) is a non-steroidal, orally bioavailable selective androgen receptor modulator (SARM). Mechanistically, it binds the androgen receptor with tissue-selective affinity, which distinguishes it from steroidal androgens. It was developed as an investigational compound by GTx, Inc. beginning in the late 1990s (ref. 1).
Ostarine remains an experimental research chemical and is supplied strictly for laboratory research. Sports Technology Labs makes no claims regarding its effects, and nothing in this listing should be interpreted as describing outcomes in humans or animals.
Important regulatory information
MK-2866 is an investigational compound. It is not approved by the FDA and is not a dietary supplement, drug, or food. Marketing it for human ingestion is unlawful.
Listed by the World Anti-Doping Agency under S1 (Anabolic Agents — Selective Androgen Receptor Modulators) and prohibited by the NCAA, banned both in- and out-of-competition (ref. 3).
In the United States, MK-2866 is not a controlled substance and may be legally purchased and possessed for laboratory research use.
Sports Technology Labs are chemical suppliers, not medical providers. We do not condone or encourage consumer use of research compounds.
Scientific references
- Narayanan R, Mohler ML, Bohl CE, Miller DD, Dalton JT. Selective androgen receptor modulators in preclinical and clinical development. Nucl Recept Signal. 2008;6:e010.
- Van Wagoner RM, et al. Chemical composition and labeling of substances marketed as SARMs and sold via the internet. JAMA. 2017;318(20):2004–2010.
- WADA Prohibited List (2025), Section S1: Anabolic Agents — Selective Androgen Receptor Modulators (SARMs). WADA.org.
Research use only. All products on this website are intended exclusively for laboratory research and development. They are not for human or animal consumption. These statements have not been evaluated by the U.S. Food and Drug Administration, and these products are not intended to diagnose, treat, cure, or prevent any disease.








